Hi everyone,
Thanks for all your comments and questions on my presentation. It is here: Hujiang Case Study-wzge5h. I welcome further questions/comments if you have any. Thanks!
Hi everyone,
Thanks for all your comments and questions on my presentation. It is here: Hujiang Case Study-wzge5h. I welcome further questions/comments if you have any. Thanks!
To complement our class discussion on the effect of standardized testing as evident in the NYC public high school entrance exam, I’d like to present a recent argument by Yong Zhao, a Chinese-born professor of education at the University of Oregon. Basically, Zhao’s argument is as follow:
Personally, I think Zhao’s argument, while solid, is nothing new under the sun. It is just a different way to ask for a cost-benefit analysis, in a more structured, legal-binding way by making it into a law like in medicine. By likening education to medicine, I think Zhao wants to raise the stake – perhaps people are not taking side effects seriously in education because it is not a matter of imminent “life-and-death” like in medicine, but perhaps it is. Education matters to the psychological and emotional well-being of a person, which I would argue that is as important as physical well-being, and psychological distress can result in physical distress.
His other point about the US emulating Asian education is more interesting given our reading this week on Chinese education, which used to emulate the US system and now is trying to forge its own path. We have touched upon “best practice” in class and that it doesn’t seem to work because each country is different, yet it seems like the countries we covered are all trying to adopt something from models they consider “successful”. What do you think about this “best practice” approach? What is the alternative? Is it inevitable to “learn” from other countries while making your own policy? If so, how do you critically integrate “best practice” to fit your own context?
Source:
“What works may hurt: Side effects in education”, Yong Zhao, Journal of Educational, Volume 18, Issue 1, February 2017. http://link.springer.com/article/10.1007/s10833-016-9294-4
Hi everyone, as I introduced myself in our first class, my name is Dai and my goal is to become a psychologist working in Asia (I’m enrolled in the psychology program at the regular Columbia, across the street from SIPA). Thus, I’d like to use this post as an opportunity to discuss mental health, which I believe is essential for academic excellence but is not adequately reflected in social and educational policies.
In 2015, Newsweek reported a striking study by Japan’s Cabinet Office that examined child suicide. The study was striking because it found that the time of high suicide corresponded with the timing of the school year: more suicides were committed in early September when school starts and in mid-April when school resumes after spring break. The study is statistically persuasive, as their data were large: they looked at 18,000 records of child suicides from 1972–2013 (41 years). For those of us who are thinking that school stress can play a role, this thought partially supported by records of child suicide notes in 2006, which cited school stress as the cause of their decisions. Research done by Hokkaido University Professor Kenzo Denda, cited in the same Newsweek article, found that in Japan, 1 in 12 elementary school-aged children, and 1 in 4 junior high school students suffer from depression. Another study showed that suicide was the leading cause of death for Japanese children age 10-19 in 2014. Taken all of these findings into account, we can see that suicide and mental health present a concern for universities because the later part of the child spectrum (age 17-19) are university age, which means a considerable amount of university students may experience mental health problems and suicidal thoughts, some of whom since a very, very early age, as Professor Denda showed that depression was presented in elementary school.
While the above findings were specific to Japan, I think it is also reasonable to assume (we will have to assume because of the lack of quality data in Asia, something Professor Lefebure mentioned in class) that other Asian countries also face the same problem. In fact, here is a summary of mental health index in Asia Pacific in 2016 reported by The Economist (however, please note that this report is commissioned by a company called Janssen Asia Pacific, which is part of the healthcare giant Johnson & Johnson so there may be private interest in methodology and findings of the report):
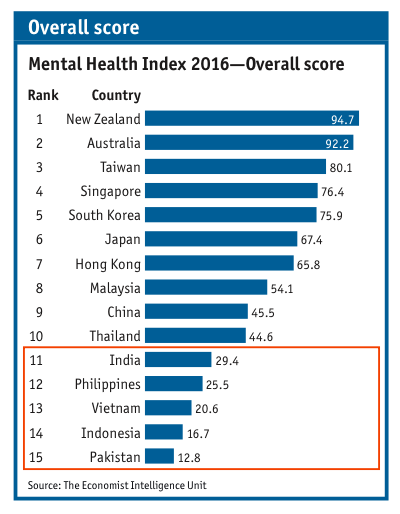
The criteria for ranking were comprised of four categories:
We could see that the ranking relatively corresponds with the economic development status of a country – more developed countries ranked higher than less-resourced countries. However, this does not mean that resource-strapped countries, those countries at the bottom of the list cannot do anything about their population with mental health. The real question is, how can they maximize their result given their limited funding? Or simply put, how can they do more with less?
With respect to higher education, what role should universities play in supporting their at-risk students and the community at large? I think education plays a key role in solving many aspects of the mental health problem. For example, universities can reduce stress by changing their curricula and non-academic initiatives. Universities can solve the lack of expert resources by training future mental health professionals. University personnel is also in a position to influence policy and public opinion.
What are your thoughts?
Sources:
Newsweek: http://www.newsweek.com/why-do-so-many-japanese-schoolchildren-kill-themselves-391648
Janssen/The Economist Report: http://www.janssen.com/apac/news-center/health-policy-and-advocacy/mentalhealthandintegration