Selecting the Initial Agent in Type 2 Diabetes
When medical nutrition therapy and exercise alone are not optimizing a patient’s glucose control, the next step is to choose an appropriate oral agent. Per the ADA, metformin, if tolerated and not contraindicated, is the preferred first agent.
The actual medication choice should incorporate a patient-centered approach, considering:
- glucose-lowering efficacy
- contraindications
- comorbidities
- patient preference
- anticipated side effects
- any concurrent drug therapy
- frequency of dose
- cost
Most endocrinologists and primary care physicians continue to prefer metformin as the optimal first-line agent, particularly in obese patients, if no contraindications are present. It has several appealing qualities:
- long safety record
- associated with improved cardiovascular outcomes in trials against sulfonylureas (Holman et al, 2008)
- inexpensive
- may assist with modest weight loss
- low risk of hypoglycemia
Combination Therapy
Half of patients on monotherapy for diabetes–even metformin–will require a second agent by three years. Meta-analyses (Bennett et al, 2011) suggest that each medication added to metformin will lower the A1C about another 1%. In some patients, first-line combination therapy may be considered sooner if the A1C is >9% before MNT has been instituted; or if the A1C remains above goal after MNT has been instituted.
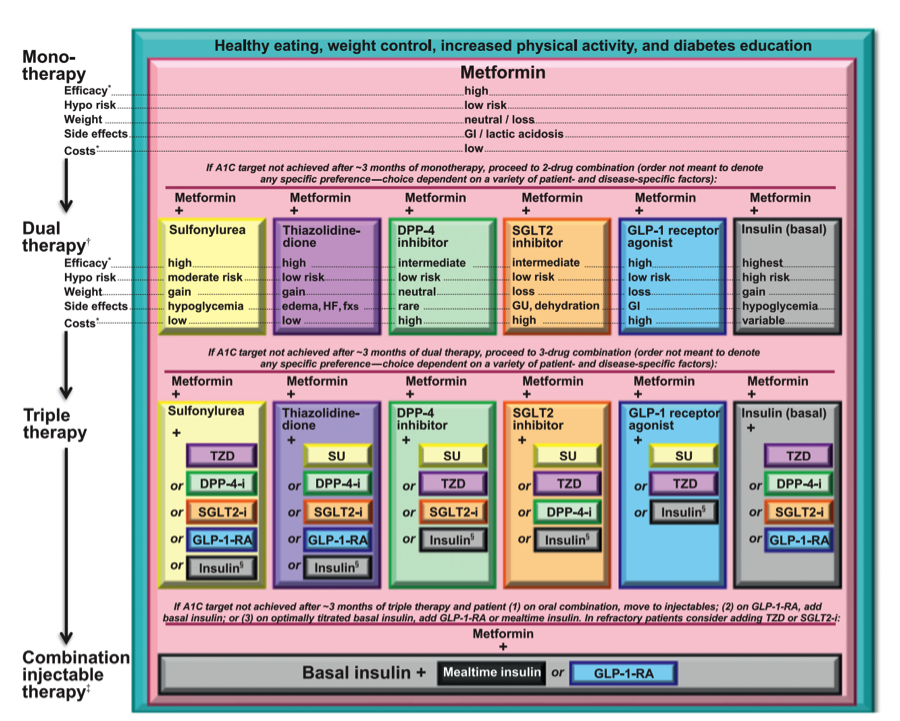
The following treatment algorithm from the 2014 ADA Standards of Medical Care combines several classes and recognizes the side effects for each class. Oral triple therapy is increasingly common in clinical practice. Nonetheless, consideration should be given as to whether a patient on triple oral therapy should actually be on insulin. If triple therapy is chosen, agents with complementary actions should be chosen, as illustrated here:
Key Points on Selecting Oral Agents
When initiating or intensifying treatment in diabetes, utilize a patient-centered approach to choosing an optimal medication regimen:
- Glycemic targets and glucose-lowering therapies must be individualized.
- Diet, exercise, and education remain the foundation of any type 2 diabetes treatment program.
- Unless there are prevalent contraindications, metformin is the optimal first-line drug.
- After metformin, there are limited data to guide us. Combination therapy with an additional 1–2 oral or injectable agents is reasonable, aiming to minimize side effects where possible.
- Ultimately, many patients will require insulin therapy alone or in combination with other agents to maintain glucose control.
- All treatment decisions, where possible, should be made in conjunction with the patient, focusing on his/her preferences, needs, and values.
- Comprehensive cardiovascular risk reduction must be a major focus of therapy.
| << Oral Agents |